
By Nicola Glover-Thomas
This report results from a one-day policy seminar in December 2017, Mental Health Tribunals: Evaluating Current Practice and Moving Forward, funded by the University of Manchester and The UK Administrative Justice Institute (UKAJI). The seminar was part of a project sponsored by UKAJI and HM Courts and Tribunals Service to explore the following issues: (i) what are the drivers for increasing detention rates under the Mental Health Act 1983?; (ii) what challenges face mental health tribunals with rising caseloads?; and (iii) what is the future for mental health tribunals?
The seminar discussion unveiled the complexity of the issues. The tension between improving efficiency within the mental health tribunal system while also maintaining a robust system of checks and balances to protect the vulnerable. It is important to have an effective system that works well and produces just outcomes. At the same time, there are practical limitations, such as limited resources and information deficits. This poses a range of challenges that require some trade-offs and compromise.
The report, ‘Mental Health Tribunals: Examining current practice, rising caseloads and future reform’, offers some reflections as to why use of the Mental Health Act 1983 is rising, particularly given the policy shift towards and reinforcement of community-focussed care following the Mental Health Act 2007. The report also considers the inextricable link between mental health legislation usage and the tribunals system. It draws upon the shared learning found within the seminar discussion to identify key issues that may be encouraging this trend, while also identifying aspects of the system that work well.
This blog post presents a summary of the findings. The full report is available below and can be downloaded here.
Mental illness costs the UK economy £100 billion a year. In 2012, the UK Government spent £126 billion on health, and pledged to spend a further £400 million on psychological therapies and mental health care provision for children and young people. Mental health needs remain acute and have garnered further support and promise for support in the years to come. Following the 2017 Autumn budget £6.3 billion of extra NHS funding was announced, of which £2.8 billion will be poured into day-to-day health services and £3.5 billion in new buildings and equipment. However, given the demands on the NHS and acute sectors overall, concerns remain that there will be little additional money for mental health.
This funding picture provides an important backdrop for considering how the mental health legislation is deployed when responding to serious mental health support needs. In the UK, the Mental Health Act 1983 (MHA 1983) (as amended by the Mental Health Act 2007) provides the legal framework which governs decisions made concerning the care and treatment of those suffering from mental disorder where they may pose a risk to themselves or others. The legislation sets out the circumstances when mental health professionals can make decisions about detention and/or treatment without the patient’s consent. The conflicting perspectives of the patient and the care provider are often the source of tension and challenge within mental health law. On the one hand, the MHA 1983 seeks to provide a workable system of checks and balances to ensure robust and justifiable decisions are made. Ensuring the interests of patients are well served is an important and fundamental driver. Yet, situated at the heart of the legislation is also the need to protect others from potential harm. Navigating through the minefield of conflicting interests is difficult; getting the balance right remains a primary goal.
Getting this right has become even more critical since the Human Rights Act 1998 which requires UK compliance with the European Convention in Human Rights. As long as a patient meets the Winterwerp criteria (Winterwerp v The Netherlands [1979] ECHR 4) detention will be lawful. The patient must reliably be shown to be of unsound mind; the mental disorder must be of a kind or degree warranting confinement; and the validity of the confinement depends on the persistence of the mental disorder. These criteria must be met in every case. Through access to a mental health tribunal, patients are offered the apparatus to review and challenge their detention. Access to and timing of a tribunal hearing is dependent upon the nature of the detention. The detention rates of these different categories will necessarily impact upon overall tribunal caseload and the level of pressure exerted upon the tribunal system. Detention rates under the mental health legislation are going up and have been doing so consistently for the last decade. This has had a knock-on effect upon tribunal applications. While there is a legal requirement to review the cases of those detained under the MHA 1983, understanding the drivers that are increasing the mental health tribunal caseload is essential.
Detention rates under the Mental Health Act 1983
The number of people detained under the MHA 1983 is rising exponentially. Overall, there were 63,600 people detained under the MHA 1983 in 2015/16 compared to 43,400 in 2005/06; an increase of 47%. The 2015/16 detention figure is the highest it has been since 2005/06 when 43,361 detentions were recorded.
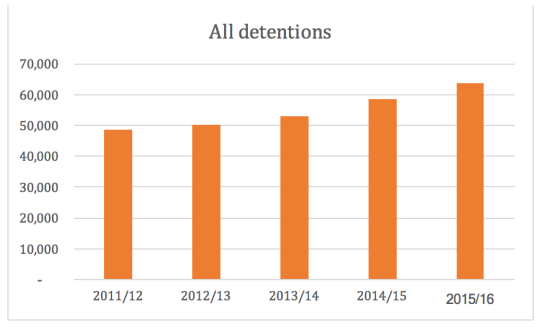
Source: NHS Digital, Inpatients formally detained in hospitals under the Mental Health Act 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, November 30, 2016
Specifically, detentions under Part II of the MHA 1983, that is section 2 admission for assessment and section 3 admission for treatment, have seen particular rises from over 28,500 in 2011/12 to nearly 39,000 in 2015/16 (nearly a 27% increase). For section 2 detentions alone, there has been a rise of nearly 32% between 2011/12 and 2015/16.

Source: NHS Digital, Inpatients formally detained in hospitals under the Mental Health Act 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, November 30, 2016
These increases have occurred at a time when both mental health and social care provision continue to experience significant financial challenges. With austerity continuing to bite, mental health provision has not always received the attention it deserves with physical health needs dominating resource allocation. However, mental health conditions account for 23% of the total burden of disease, but in terms of NHS expenditure, only 13% of health spending is currently directed towards psychiatric and related services. This under-investment is not new, and resource shortfalls continue to be commonplace. Mental health, commonly referred to as the ‘Cinderella’ service, has been struggling under the weight of systemic neglect for a considerable time. In 2016, the pressure placed upon the NHS was recognised. The provision of universal, high quality healthcare remains a steadfast commitment, but the way in which the NHS operates to meet this requires change to accommodate the modern-day context. In 2016, NHS England published a report, Five Year Forward View for Mental Health, which identified key recommendations to improve both the experience of health care and overall outcomes. The report identifies key changes that necessitate a radical rethink around healthcare provision. Notably, a central aspect of the strategy is the recognition that steps need to be taken to respond to increasing inflexibility within the NHS. This impedes the way in which health care provision is undertaken as artificial barriers, which are stymieing both policy and practical implementation, are created.
So, why are detention rates under the MHA 1983 going up? Given continued concern over the mental health tribunal’s increasing workload, what might be the underlying causes for the greater reliance upon the civil commitment procedures under the MHA? An area for concern is the rise in section 2 use. This section authorises the compulsory admission of a patient for the purpose of assessing the patient’s mental condition. Use of section 2 is thought to assist with access to mental health services. Availability of beds has decreased and bed shortages are resulting in delayed admission. With bed occupancy rates in inpatient facilities being well above recommended levels, use of voluntary admission as a preferred method of entering the mental health system is being hampered by scarce resources. Where a patient is deemed in need of care in hospital, resort to the civil commitment may be the quickest means of opening up services. The bed occupancy data for all mental health overnight beds was largely stable throughout 2017, though demonstrated a significant overall decline. Across England there are currently just over 18,000 beds available. In 2015/16 mental health beds for overnight use were in the region of 22,500. This accounted for a 20% drop in available beds between 2015 and 2017. In 2001, 34,214 overnight beds were available for use. This represents a 47% reduction of mental health beds since 2001.
Another area of concern believed to be directly impacting upon formal detention rates is the role of inequalities and cognitive bias in decision-making. Data from 2016/17 illustrates that people within a broad Black ethnic group were more likely to be detained under the MHA 1983, with those from the Black Caribbean group having the highest rate of detention of all ethnic groups. The Mental Health Act: independent review is currently underway and work is being undertaken to understand why these differential rates of detention are taking place (reporting Autumn 2018).
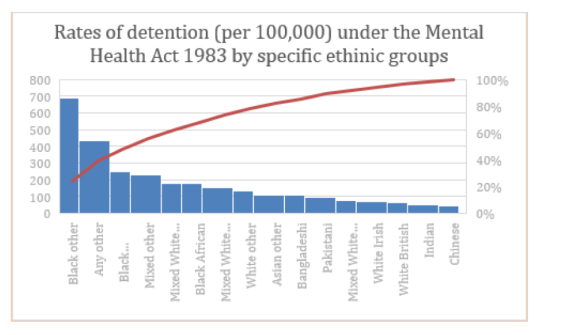
Sources: Rates of detention (per 100,000) under the Mental Health Act 1983 by specific ethnic group in England 2016/17, Mental Health Services Dataset at: http://content.digital.nhs.uk/mhsds
A further factor that has influenced the increasing utilisation of the civil commitment procedures under the MHA 1983 is the decline in contact patients experience when in the community. Evidence supports the view that a successful community care experience is one where there are strong family and social networks in place (Glover-Thomas, 2007). With less support in the community, the services available are often inadequate to meet needs and keeping patients out of acute crisis becomes increasingly difficult.
Without sufficient funding to support community-based care, accessing services for patients has required greater reliance on formal hospital detention provisions. However, the inpatient data suggests that entry into the mental health system for many continues to be through section 2. Unless the criteria for section 3 admission for treatment are met, most patients will be discharged within 28 days. For many patients this begins the pattern of repeated revolving door, short-term inpatient stays and has arguably been exacerbated by the introduction of Community Treatment Orders (CTOs) under the MHA 2007. The difficulty is that trying to determine the extent to which inpatient data includes revolving door patients is difficult. The data is not sufficiently nuanced; it does not demarcate the nature of the admission, past psychiatric history and community care experience. Constructing an accurate representation of patients entering the mental health system under the MHA 1983 is therefore difficult.
Common law developments have also influenced formal detention figures under the legislation. The Supreme Court in P v Cheshire West and Chester Council; P & Q v Surrey County Council [2014] UKSC 19 (‘Cheshire West’) clarified an ‘acid test’ for what constitutes a ‘deprivation of liberty’. The outcome of this case has significantly lowered the threshold for the engagement of Article 5 ECHR. The acid test states that an individual is deprived of their liberty for the purposes of Article 5 ECHR if they: lack the capacity to consent to their care/treatment arrangements; are under continuous supervision and control; and are not free to leave. All three elements must be present for the acid test to be met. This case has raised several fundamental questions around the concept of physical liberty and what is needed to both protect this and ensure detention is legitimate. For mental health patients, repercussions following Cheshire West have been felt. The broader impact of the decision has reinforced a cautionary approach to be adopted by clinicians. Section 131 MHA allows the informal treatment of patients with their consent. Looking at the data around informal patient numbers, a stark shift is evident following the Cheshire West decision. The number of informal patients in psychiatric facilities has gone down while formal detentions have increased. In 2008/09, there were 75,843 informal patients, while there were 30,913 formally detained patients. By 2014/15, the balance between these two categories of patient had shifted considerably, with 51,196 informal patients and 54,225 formal patients. This suggests that post-Cheshire West health and social care providers and decision-makers may be much more sensitive now to the risk of unauthorised deprivation of liberties and this has consequently had a knock-on effect upon formal detention rates.
The impact of ‘risk’ as a more nebulous construct has also been felt in recent years in the mental health care field. Historically, risk has always featured prominently in mental health care. Following the MHA 2007, risk assessment and management have become the explicit concerns of the civil commitment process. Mental health decision-makers must seek to achieve a balance between their patients’ personal freedoms and the public’s safety. Risk provides a mechanism (though an albeit problematic one) with which decision-makers may achieve this balance, by deploying the compulsory powers under the MHA where a patient’s level of risk becomes so great that he/she poses a threat to either him/herself or others. The standards which the compulsory criteria require are ambiguous. Decision-makers enjoy a wide discretion to interpret relevant factors according to their professional judgment. Increasing caution around risk in terms of understanding what it is, how to assess it and manage it accurately and effectively is increasingly evident within mental health care practice. Behavioural responses to this have also been shaped by external influences, of which the Cheshire West case is one.
Two further cases involving the assessment of suicide risk have also had an impact upon risk and its management regarding clinical decision-making. In Savage v. South Essex Partnership NHS Foundation Trust [2008] UKHL 74, failures to take reasonable precautions to protect the lives of patients with suicidal thoughts were found to have violated Article 2 ECHR. In Rabone v. Pennine Care NHS Foundation Trust [2012] UKSC 2, the Court held that the operational duty to protect life could be owed to informal psychiatric patients as well as formally detained patients under the MHA 1983 (Allen, 2013) as long as there has been ‘an assumption of responsibility by the State for the individual’s welfare and safety (including by the exercise of control)’.
Another factor pushing detention rates up is increased used of section 136 MHA 1983 by the police. They have powers to remove a person to a place of safety or to keep a person in an existing place of safety where it is believed the person needs to be examined by a doctor. Although there is a presumption that resort to the MHA should be a last resort, a shift in the use of section 136 by the police is apparent.
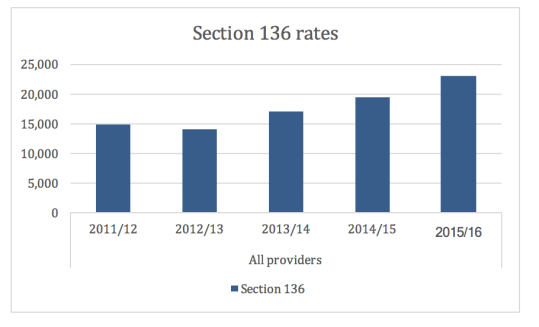
Source: NHS Digital, Inpatients formally detained in hospitals under the Mental Health Act 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, November 30, 2016.
More notably, the shift in section 136 reliance has impacted on conversion rates. With the presumption that section 136 should only ever be used if no other avenues were available, conversion rates from section 136 to section 2 and section 3 were high. Since the early 2000s conversion rates were in the region of 85%, suggesting that the police were primarily putting people on a section 136 who warranted informal admission to hospital. Those taken out of a public place by the policy were highly likely to need mental health support. However, since the Cheshire West decision, which has since discouraged use of the informal patient status under section 131, the increasingly heavy use of section 136 is likely to have an impact on section 2 and 3 figures. Since 2014, conversion rates from section 136 to both section 2 (29% increase since 2014) and section 3 (32% increase since 2014) have risen. Although drawing a firm conclusion that the Cheshire West decision has had a marked and direct effect on conversion rates is difficult given the presence of multi-factorial drivers, it has certainly played a significant role.

Source: NHS Digital, Inpatients formally detained in hospitals under the Mental Health Act 1983 and patients subject to Supervised Community Treatment: 2015/16, Annual figures, November 30, 2016.
This data suggests a number of things. First, the use of section 136 has gone up, as has the conversion rate from section 136 to sections 2 and 3. Therefore, there is a direct bearing upon overall detention figures and consequently tribunal receipts. Second, evidence suggests that revolving door patients are being identified by police and section 136 is being used. Third, the Care Quality Commission’s concern that community-based services are becoming increasingly fragmented (CQC, 2015) with more gaps forming in service provision may be requiring greater input by the police. Finally, concerns around patients either not being able to access mental health services when they need it or being discharged too quickly because of overstretched acute care services, may be leading to more vulnerable people on the streets which the police are having to identify and support. This data provides a useful insight into the fragile nature of the contemporary mental health system and impact of this on mental health tribunal activity.
Mental Health Tribunal Caseloads
The detention data presents a picture of increasing demand upon a strained mental health system. Reasons behind the upsurge in inpatient detention under the MHA 1983, as discussed above, have had a knock-on effect upon the case review process. Between 2007/8 and 2016/17, tribunal receipts have risen by over 33%, increasing from nearly 22,000 to more than 33,000 receipts in 2016/17.

Source: Data taken from: Ministry of Justice, Tribunals and gender recognition certificate statistics quarterly – July to September 2017, London, Ministry of Justice, 2017.
Section 2 appeals are rising in volume at around 32%, though this also reflects the rising volume of section 2 detentions (a rise of nearly 32% between 2011/12 and 2015/16). Section 2 applications increased from 9,729 in 2014/15 to 10,093 in 2015/16, while hearings increased by over 7%. Whereas, section 2 discharges made by tribunals dropped by approximately 1.5% over the same period (CQC, 2015).
With the increase in overall activity, mental health tribunal workload presents significant practical challenges and has downstream cost implications especially for the Ministry of Justice. Section 2 review applications, in particular, have raised specific problems. Section 2 hearings must be listed within 7 days of application, and the hearing must be undertaken within 14 days beginning with the date of admission. With the pressure on time and mounting demands to make effective and efficient decisions, the increasing number of section 2 applications has meant that mental health tribunals have had to manage this while maintaining standards. Effective decision making may be affected by the level of information, data and supporting documentation available at the hearing. The short timeframe to prepare a case may result in the quality and depth of the accompanying responsible authority reports being compromised. There may have been insufficient time for the clinical team to be in a position to make a judgement about the patient’s current mental state. Treatment options may not have had enough time to provide an indicative picture of potential success. For many cases, writing a report about a patient for whom the clinical team still knows little will be difficult. Added to this is the often-chronic demand for reports to be produced quickly and at short notice. With insufficient information, projected treatment outcomes unknown and little time for the patient to settle, both the clinical team and tribunal panel are faced with a decision-making situation that is fraught with difficulty and necessarily encourages a cautious approach.
Despite the practical constraints mental health tribunals sometimes face, tribunals provide patients with a number of helpful opportunities. Importantly, patients are provided with a chance for their voice to be heard. The hearing provides a chance for the patient’s case to be reviewed and for them to speak about their experiences. For many patients, discharge from hospital may not be the goal, but a tribunal hearing provides a forum to scrutinise the patient’s progress, consider next steps and evaluate the patient’s continuing needs. Importantly, the tribunal hearing acts as a protective mechanism to safeguard the patient.
Since the introduction of Independent Mental Health Advocates (IMHAs) under the MHA 2007, access to some form of independent legal support and representation has been strong. Most detained patients know that they are entitled to legal support; however, accessing high-quality legal provision may not necessarily be a universal experience by patients. IMHAs offer a valuable bridge between the patient, lawyers and the clinical environment. Independent advocacy increases the patient’s self-determination and provides a mechanism to support patients present a more holistic picture of their current state of health. However, despite the valuable contributions made by IMHAs, many practical challenges remain, including delays, problems with the pre-hearing medical examination and difficulties around the availability of private space for tribunal hearings in hospitals.
The Ministry of Justice’s Transforming Justice plan published in 2016 (MoJ, 2016) sets out a far-reaching plan for court reform with technology and innovation as its heart. Scope for technology in the mental health tribunal system is evident and may have a valuable impact in overcoming some of the practical difficulties experienced by panels and patients on a regular basis. Despite the benefits that may come from greater use of technology, there is a need to be mindful of the particular vulnerability of individuals being formally detained and being seen by mental health tribunals. There is a clear tension between the focus on efficiency and ensuring legal safeguards and protections are maintained.
This issue is particularly evident when examining the question of whether cases should be examined orally or on the papers. Studies examining other tribunals systems have considered the debate (Thomas, 2017). Oral hearings offer the benefit of the tribunal panel meeting the patient. In addition to the medical reports and other paper evidence supplied as part of the hearing process, the tribunal panel have an opportunity to hear direct evidence given by the patient themselves. Hearing a case on the papers loses much of this exchange. A tribunal will only be able to base a decision on the paper evidence submitted and there will be no opportunity to interrogate this evidence further. Within mental health, paper hearings without the patient present do take place. For example, in 2016/17, out of 4,645 applications against CTOs, 520 of those were undertaken on the papers only. Taking account of the withdrawn applications, this figure represents nearly 14% of these types of hearings during this period. Paper hearings do aid timeliness and assist with the goal of driving up efficiency. However, as Thomas observes, oral appeals are more commonly allowed compared to those heard on the papers.
Demand for reform within the mental health tribunal system is mounting, but in order to respond to the challenge of increasing caseloads, it is important to ensure reforms are informed by evidence. More research is essential. Improving efficiency within the mental health tribunal system is not an easy task. This is largely because the tribunal system should not be viewed in a vacuum. Tribunal caseloads are inextricably linked to initial decisions to detain under the MHA 1983. While detention rates (under all relevant provisions) are high and getting higher, the impact will be felt by mental health tribunals. Looking forward, it is important to understand better why greater reliance is being placed upon the MHA, and what, if anything can be done to resolve this. Undertaking empirical research into this is essential.
References
N. Allen, ‘The right to life in a suicidal state’ International Journal of Law and Psychiatry (2013) 36 (5-6), p350-357 (CQC, 2015).
N. Glover-Thomas, ‘Joint Working; Reality or Rhetoric in Housing the Mentally Vulnerable?’ Journal of Social Welfare and Family Law (2007) 29(3-4), p217-233.
The Mental Health Taskforce, The Five Year Forward View for Mental Health A report from the independent Mental Health Taskforce to the NHS in England, February 2016.
Ministry of Justice, ‘Transforming Our Justice System by the Lord Chancellor, the Lord Chief Justice and the Senior President of Tribunals’, September 2016. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/553261/joint-vision-statement.pdf
R. Thomas, ‘Oral and paper tribunal appeals, and the online future’, January 2017. Available at: https://ukaji.org/2017/01/31/oral-and-paper-tribunal-appeals-and-the-online-future/
About the author:
Nicola Glover-Thomas is Professor of Medical Law at the School of Law, University of Manchester.

Discussion
No comments yet.